Crohn’s Disease
What is Crohn’s Disease?
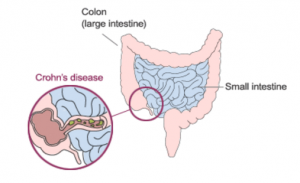
Crohn’s disease is a chronic disorder that causes inflammation of the (GI) tract. Although it can involve any area of the GI tract from the mouth to the anus, it most commonly affects the small intestine and/or colon. Crohn’s and a related disease, ulcerative colitis, are the two main disease categories that belong to a larger group of illnesses called inflammatory bowel disease (IBD).
What Are The Causes of Crohn’s Disease?
We do not yet know what causes this disease. Studies indicate that the inflammation in Crohn’s disease involves a complex interaction of factors: the genes the person has inherited, the immune system, and something in the environment. Foreign substances (antigens) in the environment may be the direct cause of the inflammation, or they may stimulate the body’s defenses to produce an inflammation that continues without control.
In patients with Crohn’s disease, once the patient’s immune system is “turned on,” it does not know how to properly “turn off.” As a result, inflammation damages the intestine and causes the symptoms of Crohn’s disease. One of the major goals of medical therapy is to help patients regulate their immune system better.
What Are The Signs And Symptoms of Crohn’s Disease?
Symptoms of Crohn’s disease include persistent diarrhea (loose, watery, or frequent bowel movements), crampy abdominal pain, fever, fatigue, and, at times, rectal bleeding. Symptoms vary from person to person and may change over time. Loss of appetite and subsequent weight loss also may occur. Of note is that the disease is not always limited to the GI tract; it can also affect the joints, eyes, skin, and liver. Some patients may develop tears (fissures) in the lining of the anus, which may cause pain and bleed, especially during bowel movements. Chronic, severe inflammation may also cause a fistula to develop. A fistula is a tunnel that leads from one part of the intestine to another, or that connects the intestine to the bladder, vagina, or skin. Fistulas occur most commonly around the anal area. If this complication arises, you may notice drainage of mucus, pus, or stool from this opening.
Symptoms may range from mild to severe. Because Crohn’s is a chronic disease, patients may go through periods in which the disease flares up, when the disease is active. These episodes are often followed by times of remission when the symptoms disappear or decrease. In general, people with Crohn’s disease lead full, active, and productive lives.
What Are Risk Factors of Crohn’s Disease?
Crohn’s and a related disease, ulcerative colitis, are the two main disease categories that belong to a larger group of illnesses called inflammatory bowel disease (IBD). It is estimated that as many as one million Americans have IBD — with that number evenly split between Crohn’s disease and ulcerative colitis. Males and females appear to be affected equally. Crohn’s disease may occur in people of all ages, but it is primarily a disease of adolescents and young adults, affecting mainly those between the age of 15 and 35. However, it can also occur in people outside this age group.
IBD tends to run in families. Studies have shown that about 20 to 25 percent of patients may have a close relative with either Crohn’s or ulcerative colitis. If a person has a relative with the disease, his or her risk is about 10 times greater than that of the general population. If that relative happens to be a brother or sister, the risk is 30 times greater. There is no way to predict which, if any, family members will develop Crohn’s disease.
IBD is more commonly found in certain ethnic groups. American Jews of European descent are four to five times more likely to develop IBD than the general population. IBD has long been thought of as a disease predominantly affecting Caucasians. However, there has been a steady increase in reported cases of both Crohn’s disease and ulcerative colitis among African Americans. The prevalence rates among Hispanics and Asians are lower than those for Caucasians and African Americans.
How is Crohn’s Disease Diagnosed?
There is no single test that can confirm the diagnosis of Crohn’s disease. Doctors rely on a combination of the patient’s history and physical exam, results of laboratory tests, X-rays (small bowel series), colonoscopy and recently, small bowel capsule endoscopy. Crohn’s disease often mimics other condition.
What Are Possible Treatments For Crohn’s Disease?
Medications Used to Treat Crohn’s Disease
Currently, there is no cure for Crohn’s disease. The goal of medical treatment, therefore, is to modulate the inflammatory response. Several groups of drugs are used to treat Crohn’s disease today. They are:
- Aminosalicylates (5-ASA): These medications typically are used to treat mild to moderate symptoms.
- Corticosteroids: These drugs have significant short- and long-term side effects and should not be used as a maintenance medication.
- Immune Modifiers: Azathioprine (Imuran®), 6-MP (Purinethol®), and methotrexate are used to help decrease corticosteroid dosage and also to help heal fistulas. In addition, immune modifiers can help maintain disease remission.
- Antibiotics: metronidazole, ciprofloxacin, rifaximin (Xifaxan®)
Biologic therapies
Infliximab (Remicade®), adalimumab (Humira®), certolizumab pegol (Cimzia®), natalizumab (Tysabri®). These medications are used for inducing and maintaining clinical response and remission in adult patients with moderately to severely active Crohn’s disease who have had an inadequate response to or are unable to tolerate, conventional Crohn’s disease therapies.
Role of Surgery
Two-thirds to three-quarters of patients with Crohn’s disease will require surgery at some point during their lives. Surgery becomes necessary in Crohn’s disease when medications can no longer control the symptoms. It may also be performed to repair a fistula or fissure. Another indication for surgery is the presence of intestinal obstruction or other complication, such as an intestinal abscess. Surgery is not considered a cure for Crohn’s disease, because the disease frequently recurs at or near the site where the intestine has been reattached (anastomosis). The overall goal of surgery in Crohn’s disease is to conserve bowel and return the individual to the best possible quality of life.
Steps to Help With Crohn’s Disease
Nutrition
There is no evidence that any particular foods cause or contribute to Crohn’s disease. Paying special attention to diet may help reduce symptoms, replace lost nutrients, and promote healing.
When Crohn’s disease is active, soft, bland foods may cause less discomfort than spicy or high-fiber foods. Except for restricting milk in lactose-intolerant patients, most gastroenterologists try to be flexible in planning the diets of their Crohn’s patients. A healthy diet should contain a variety of foods from all food groups. Meat, fish, poultry, and dairy products (if tolerated) are sources of protein; bread, cereal, starches, fruits, and vegetables are sources of carbohydrate; margarine and oils are sources of fat.
Emotional Factors
There is no evidence to show that stress, anxiety, or tension is responsible for Crohn’s disease. However, they may contribute to an exacerbation of the disease. The emotional distress that patients sometimes feel may be a reaction to the symptoms of the disease itself. Although formal psychotherapy is generally not necessary, some patients are helped considerably by speaking with a therapist who is knowledgeable about IBD or about chronic illness in general.


